
I quote directly from the Twitter feed of Anthony Scaramucci, @scaramucci:
“@dhank2525 agree. We already have Univ Health Care, we made decision long ago to treat everyone that enters an emergency room.”
Mr. Scaramucci is President Trump’s Communications Chief, replacing Sean Spicer. Mr. Scaramucci is neither veteran journalist nor healthcare policy wonk. He’s a successful businessman, which I respect for his savvy and ability to build a fund, attract investors, and create a media persona which he has telegenically broadcast on CNBC and elsewhere over the past decade. He’s got a engaging public personality, and goes by the moniker, “Mooch.”
But as brilliant a businessman as Mooch is, and he is, Mooch’s pronouncement that an ER is equivalent to universal healthcare is so not true, it’s an un-fact. It’s just wrong, and wrong on many levels. And from his businessman’s point-of-view, I want Mooch to know there’s a real return-on-investment (ROI, a concept he’ll appreciate) for funding preventive care and, especially, boosting funding for the social determinants of health which bolster individual, population (say, for a group of people diagnosed with Type 2 diabetes or heart failure), and public health (at the community level).
In sum: ERs are expensive, too expensive for delivering primary care, and too late in health citizens’ lives for supporting prevention and early diagnosis. Let’s review some solid evidence on the ROI of spending more on primary care and the social determinants of health (SDOH).
 Save by spending more on primary care. The rest of the developed world, those OECD nations (to any one of which Mr. Scaramucci, reportedly, would have liked an ambassadorship), all allocate much more spending per capita to primary care than the U.S. does. A strong primary care backbone is the on-ramp to health care and self-care literacy and competency, and costs the system (and taxpayers) less “earlier” than spending “later” when medical conditions and diseases emerge. Here’s some recent research from the successful business people at PwC on primary care in the New Health Economy. Here’s another view on the importance of primary care in developed economies from The Commonwealth Fund which provides additional insights into the ROI of primary care in countries that have mindfully made the investment in that national primary care backbone.
Save by spending more on primary care. The rest of the developed world, those OECD nations (to any one of which Mr. Scaramucci, reportedly, would have liked an ambassadorship), all allocate much more spending per capita to primary care than the U.S. does. A strong primary care backbone is the on-ramp to health care and self-care literacy and competency, and costs the system (and taxpayers) less “earlier” than spending “later” when medical conditions and diseases emerge. Here’s some recent research from the successful business people at PwC on primary care in the New Health Economy. Here’s another view on the importance of primary care in developed economies from The Commonwealth Fund which provides additional insights into the ROI of primary care in countries that have mindfully made the investment in that national primary care backbone.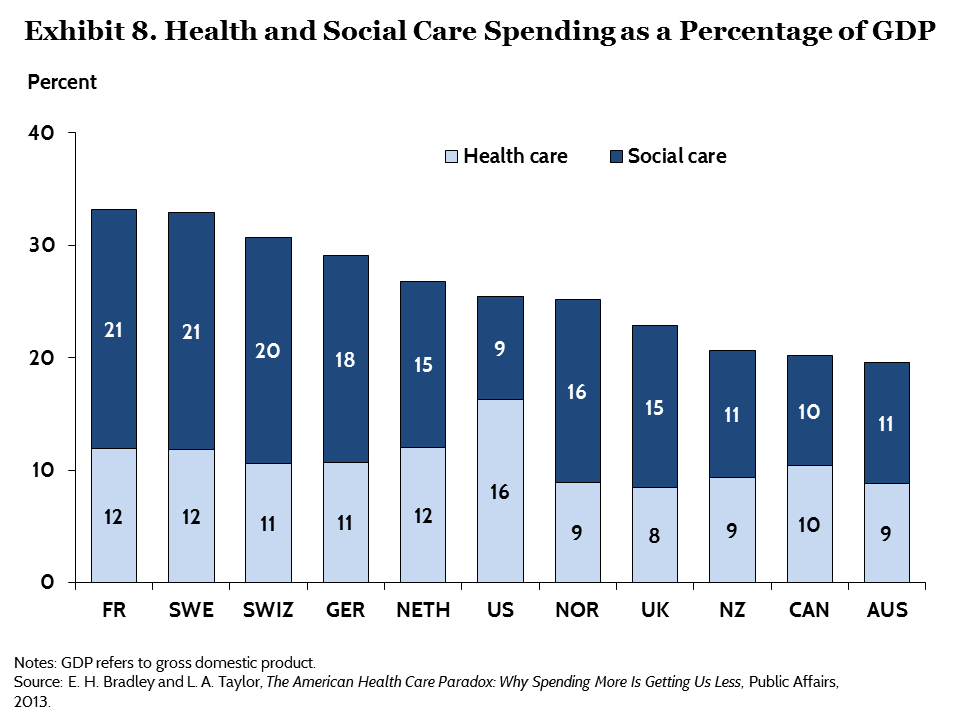 Save by spending more on social care. Those wealthy nations also spend more on social care per capita, like education and housing. Early childhood education is a building block to literacy, health literacy, good jobs, and a civil society. Safe and clean housing also boosts health: that could be a sound argument for the appointment of Dr. Ben Carson as Secretary of Housing and Urban Development (HUD). Here’s a meta-analysis on the direct correlation between social spending and health outcomes published in the policy journal Health Affairs. For further learning on this key issue, here’s a link to work from The Robert Wood Johnson Foundation on how spending on social care has an ROI for peoples’ health outcomes. Here’s the money quote you will surely appreciate: when comparing state-to-state spending, a 20% change in median social-to-health spending was associated with 85,000 fewer adults with obesity and 950,000 fewer adults with mental illness. Allocating more funding to housing and nutrition were found to be particularly impactful.
Save by spending more on social care. Those wealthy nations also spend more on social care per capita, like education and housing. Early childhood education is a building block to literacy, health literacy, good jobs, and a civil society. Safe and clean housing also boosts health: that could be a sound argument for the appointment of Dr. Ben Carson as Secretary of Housing and Urban Development (HUD). Here’s a meta-analysis on the direct correlation between social spending and health outcomes published in the policy journal Health Affairs. For further learning on this key issue, here’s a link to work from The Robert Wood Johnson Foundation on how spending on social care has an ROI for peoples’ health outcomes. Here’s the money quote you will surely appreciate: when comparing state-to-state spending, a 20% change in median social-to-health spending was associated with 85,000 fewer adults with obesity and 950,000 fewer adults with mental illness. Allocating more funding to housing and nutrition were found to be particularly impactful.
I’ll be speaking in San Diego at 7 am this Friday morning, 28th July 2017, at the Equity of Health breakfast, part of the American Hospital Association Leadership Summit. I’d love to welcome you to the talk, during which I’ll discuss my work marrying health economics to health care disparities. This work was first inspired and informed with visceral and vivid memories of being a child in suburban Detroit on July 23, 1967 — this week, marking the 50th anniversary of the Detroit riots.
Health Populi’s Hot Points: If you remember one thing from this post, Mooch, consider this: our ZIP code is more important than our genetic code when it comes to health status. Some of us were born to families with good jobs that came with health insurance (perhaps like your family on Long Island or mine in suburban Detroit); our parents sent us kids on to excellent higher education (like you to Wharton and Harvard, and me to the University of Michigan). How lucky are/were we?
Other peoples’ ZIP codes haven’t afforded them access to these social determinants of health that, together, help ensure (with an “e,” not an “i”) and set the table for good health and literacy for a good life. That’s the kind of life that shapes our ability to pursue Life, Liberty, and Happiness. You and I both want that for the health citizens of the United States of America.
My job at THINK-Health is to inspire thinking across and among the broad health and healthcare ecosystem stakeholders, from care providers and health insurance plans to pharma and technology, food, consumer goods and electronics, and financial services. I write this to inspire Mooch in considering the opportunities for investing in health, to prevent more unneccessary and ineffective healthcare spending (in the ER) too late to get the ROI on healthy American lives.


 Interviewed live on BNN Bloomberg (Canada) on the market for GLP-1 drugs for weight loss and their impact on both the health care system and consumer goods and services -- notably, food, nutrition, retail health, gyms, and other sectors.
Interviewed live on BNN Bloomberg (Canada) on the market for GLP-1 drugs for weight loss and their impact on both the health care system and consumer goods and services -- notably, food, nutrition, retail health, gyms, and other sectors. Thank you, Feedspot, for
Thank you, Feedspot, for  As you may know, I have been splitting work- and living-time between the U.S. and the E.U., most recently living in and working from Brussels. In the month of September 2024, I'll be splitting time between London and other parts of the U.K., and Italy where I'll be working with clients on consumer health, self-care and home care focused on food-as-medicine, digital health, business and scenario planning for the future...
As you may know, I have been splitting work- and living-time between the U.S. and the E.U., most recently living in and working from Brussels. In the month of September 2024, I'll be splitting time between London and other parts of the U.K., and Italy where I'll be working with clients on consumer health, self-care and home care focused on food-as-medicine, digital health, business and scenario planning for the future...