
 Overuse of health care is defined as the delivery of health care services for which the risks outweigh the benefits, according to a study into the utilization of ambulatory care health services published in the January 28, 2013, issue of JAMA Internal Medicine (the new title for the Archives of Internal Medicine). “Trends in the Overuse of Ambulatory Health Care Services in the United States” found that, of the estimated $700 billion that is wasted annually in U.S. health care, overuse comprises about $280 billion – over one-third of waste — equal to over 10% of total health spending in the nation.
Overuse of health care is defined as the delivery of health care services for which the risks outweigh the benefits, according to a study into the utilization of ambulatory care health services published in the January 28, 2013, issue of JAMA Internal Medicine (the new title for the Archives of Internal Medicine). “Trends in the Overuse of Ambulatory Health Care Services in the United States” found that, of the estimated $700 billion that is wasted annually in U.S. health care, overuse comprises about $280 billion – over one-third of waste — equal to over 10% of total health spending in the nation.
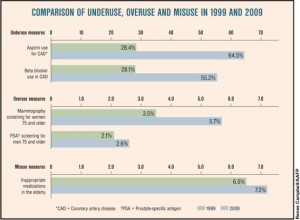
Overuse of health care falls into several categories, including over-testing (e.g., imaging), defensive medicine, use of certain prescription drugs (e.g., antibiotics), and other services.
 This wasteful, and often dangerous, phenomenon was highlighted by Shannon Brownlee’s seminal work, Overtreated, which I wrote about here on right-sizing health care.
This wasteful, and often dangerous, phenomenon was highlighted by Shannon Brownlee’s seminal work, Overtreated, which I wrote about here on right-sizing health care.
The JAMA study found that clinical practice guidelines for physicians have largely focused on the “underused” portion of waste, not so much the overtreatment aspect. According to the research, there were only limited reductions in inappropriate care between 1999 and 2009.
“Reducing health care costs and improving the quality of care in the United States can be achieved by reducing overuse and misuse of health care services, but it will require making uncomfortable decisions that patients, physicians and policymakers have been historically unwilling to make,” the authors wrote. “Developing clinical practice guidelines that define when care should not be delivered and performance measures to address inappropriate care are critical steps to advance the mission of increasing the value and efficiency of health care delivery.”
The ABIM Foundation, which represents dozens of physician professional associations, business coalitions, unions and consumer advocacy groups, developed the Choosing Wisely campaign to educate health providers and consumers about rational decision making when it comes to health care and quality improvement. The campaign has identified areas that physicians could broach with patients with the objective of stemming unnecessary tests. For example, the American Academy of Family Practice developed an initial list of five areas that are commonly tested but often harmful and unnecessary:
- Imaging for low back pain
- Antibiotics for acute short-term sinusitis
- DEXA screening for young patients
- EKGs for asymptomatic, low-risk patients
- Pap smears for young or low-risk women.
More information on the Choosing Wisely effort can be found here.
Health Populi’s Hot Points: Why worry about overtreatment? Aside from the fact that the practice can be very harmful to the individual patient, and broader public health outcomes, it’s bloody expensive. In a nation spending nearly $3 trillion on health care, with health being the #1 long-term deficit driver, addressing the 10% component that is waste could yield hundreds of billions of dollars that could be re-deployed in a variety of ways…such as reducing said deficit.
But reducing overtreatment will be complicated, and don’t blame only the physicians’ concern about defensive medicine. Note that we consumers in American like shiny new things that are expensive — especially when it seems we’re not actually paying for them. In stunning research published in the February 2013 Health Affairs issue devoted to patient engagement, Focus Groups Highlight That Many Patients Object to Clinicians’ Focusing on Costs, it appears that U.S. health consumers aren’t too open to the idea of discussing costs with physicians “in the clinical encounter,” the authors say.
The research identified four key barriers to peoples’ willingness to weigh health care costs:
- Preference for the “best” care option, regardless of cost – say preference for an MRI (higher cost) vs. a CT scan (lower cost) although the marginal benefit could be nil;
- Inexperience making trade-offs between health and money;
- Lack of interest in costs borne to society at large because of lacking understanding of how health insurance ‘works’ including “disdain” for insurance companies and lack of perceived personal responsibility for cost control; and,
- The dilemma of “The Commons.” (If you didn’t learn about this in your Economics 101 course, pls view this Khan Academy explanation which does a wonderful job articulating the “tragedy”).
The authors conclude that, “public attitudes about health care costs must undergo a significant shift.” Some of this has begun to happen with the growth of consumer-directed health care, where consumers have more “skin in the game” of health financing. Note that the study population in these focus groups included only people with health insurance, who have been largely shielded from high deductibles, copays, and self-pay experiences. Their experiences will undergo big changes in the coming months and years. Within 5 years, most insured Americans will get a taste of the consumerization of health care. It will be heavy lifting in the interim, and communicating how to use benefits and the individual patient’s responsibility will require brilliant communication skills from payers and plan sponsors — namely, employers and the government.


 I'm gratified to be named on
I'm gratified to be named on  I’m celebrating America’s 250th birthday both patriotically and professionally, honored that the NLM included my 2010 paper, “How Smartphones Are Changing Healthcare for Consumers and Patients” as one of 250 items curated for the digital archive of 250 Years of American Medicine.
I’m celebrating America’s 250th birthday both patriotically and professionally, honored that the NLM included my 2010 paper, “How Smartphones Are Changing Healthcare for Consumers and Patients” as one of 250 items curated for the digital archive of 250 Years of American Medicine.