
In researching several .gov websites from last Monday 20th January 2025, I had an ongoing frustrating user experience in being faced with “404 Error” messages like this one from WhiteHouse.gov.
“President Trump’s First Week Hammered Public Health,” Dr. Arthur Kellerman, an ER doc, public health researcher, and patient advocate asserted in Forbes yesterday:
“For now, the only health communications Americans receive will come from sources outside the government, such as professional societies, non-governmental organizations, advocacy groups, and businesses, vaccine skeptics, conspiracy theorists, foreign agents and bots posing as Americans to spread disinformation. It will be up to us to figure out what to believe.”
Now a week later, into week 2 of President Trump and team’s assumption of the White House and sorting through dozens of executive orders pertinent and adjacent to health and health care, I have to ask the question: can the private sector fill in for public sector health information gaps?

In figuring out how I could get my work done last week, I learned that the new administration had put an immediate pause on, “anything intended to be published in the Federal Register, where the executive branch communicates rules and regulations, and the Morbidity and Mortality Weekly Report, a Centers for Disease Control and Prevention scientific publication,” based on an official memo obtained by the AP. (FYI, I click into MMWR and CDC publications at least once a day for my work flow and ongoing research). These sites include those under the domain of the Department of Health and Human Services including the NIH and the FDA — the latter of which informs us every day on food safety issues — say, eggs, milk, produce, and deli meats all of which have been top-of-mind in recent months.
By Friday the 24th, after four days of dealing with many digital shut doors to Federal government health information and other sources, I saw that the Wall Street Journal referred to President Trump’s list of executive orders as, “shock therapy.”
Just focusing on my wheelhouse on health, health care, and public health in the WSJ story, I quote from Lia Essley Whyte and Scott Patterson:
“New leadership at the Department of Health and Human Services halted all external communications from the health agencies through Feb. 1. Food and Drug Administration employees scrambled to clarify that they could still issue critical safety alerts, while scientists said their grant-review meetings had been canceled, potentially endangering funding for their health research. National Institutes of Health scientists were also told to stop purchases of supplies, essentially bringing their research to a halt, two people familiar with the matter said…CDC trackers on seasonal flu and bird flu hadn’t been updated, and the agency’s flagship weekly report, which has communicated public-health information for decades, wasn’t issued as normal on Thursday.”
This begs the question titling this post: can the private sector fill in the data gaps caused by the Federal public sector health information blackout?
The answer is “no.” But the private sector is still crucial to support people in self-care across peoples’ health-lives, staying well and caring for acute conditions at home. The private sector can’t solve the problem of invisibility of public goods (defined below in the Hot Points). For context and consideration, let’s re-visit a report from McKinsey published in November 2024 on health media. The content feels quite prescient today.

“Consumers are more actively engaged than ever in the health ecosystem,” the report explains. “They are quick to research preventions, symptoms, conditions, and treatments; they expect the information they receive to be relevant and high-quality; and they are ultrasensitive to engagement that seems overly familiar. In other words, they show up in the healthcare space in the same ways they do in other walks of life, from home decorating to traveling to banking.”
The McKinsey report identifies several non-governmental information sources from health care providers and systems including Cleveland Clinic, Kaiser Permanente, Mayo Clinic, and Northwell Health, among other health care organizations. In this analysis, McKinsey calculates that a health system sized at $10 billion could generate a minimum $50 million contribution margin run rate within five years through placed advertisements patients would encounter in their “end-to-end consumer healthcare journey.”
For consumers to engage with these health media sources, it takes trust. In McKinsey’s 2024 US Health and Wellness Content Survey, 3 in 4 consumers said they connected with health and wellness content at least once a week across various channels,
But the lack of trust and growing prevalence of mis-information militate against consumers’ engagement with (good) content. Just one data point of many to note: that 30 to 40% of posts about conditions, diets, or medical treatments shared on social media contained misinformation.

In fact, many consumers in the U.S. are interested in engaging with ads about health care — but this is not a universally welcome phenomenon, and it’s also specific to certain kinds of information. At the top of consumers’ list of ad-based content for health journeys, we see health care services such as imaging and lab services, health and wellness products (vitamins/minerals/supplements, over-the-counter products), and fitness in third place. The bar chart here presents the data from McKinsey’s 2024 survey to give you a sense of where health consumers value ad-based medical content.
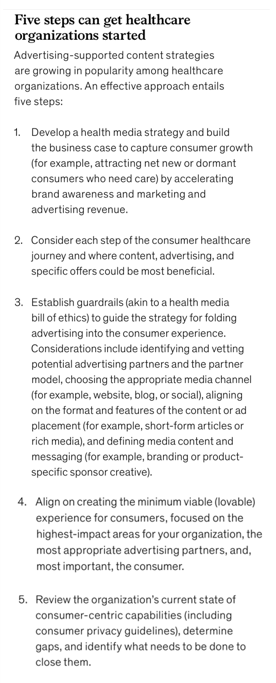
For nongovernmental (private sector) organizations to serve up advertising-supported health content, the McKinsey team offers five recommendations to keep in mind. I’ll focus here on #3 and #5, which most tightly focus on a “health media bill of ethics” or guardrails that could bolster trust-bridges between the information supplier and the consumer-as-health-citizen.
Keeping ethics- and privacy-by-design top-of-mind and across the development through implementation path would provide a True North for the organization’s team members to stand with. Clearly communicating these principles to patients and prospective users of the information/portal/service would demonstrate transparency and a shared spirit of health community.
Using these filters for picking collaborators for content and distribution would further build trust and even love-bridges between providers and users of the health media — as McKinsey’s team writes the tactic in #4 to, “align on creating the minimum viable (lovable) experience for consumers, focused on the highest-impact areas for your organization, (and) the most appropriate advertising partners….”
Health Populi’s Hot Points: Say hello to Fred Trotter, longtime health tech advocate and my first teacher on Big Data a long, long time ago. Fred has committed his amazing career focused on health data, clinical informatics, and patients’ right to access….nothing about me without me, one of our mantras over the years.
Fred is wearing one if his several t-shirts from a wardrobe of graphic tees he has curated for attending meetings, this one associated with the Robert Wood Johnson Foundation Unscripted series. The quote goes, “For science to be a public good, it has to be public.”
There are some things in life that are public by their very nature: consider Public Goods in Everyday Life, an economics book published in 2024 at Tufts University Global Development and Environment Institute.
As Martin Wolf, Chief Economics Commentator of the Financial Times, explains in the prologue, “The history of civilization is a history of public goods….The more complex the civilization the greater the number of public goods that needed to be provided. Ours is far and away the most complex civilization humanity has ever developed. So the need for public goods….such as education and health — is extraordinarily large.” 
Later in the book, author June Sekera discusses the invisibility of public goods — such as food poisonings avoided, epidemics that don’t arise or spread, and plane crashes avoided that don’t occur.
Health data that cover the complete U.S. (and world) population fall into this category of invisible public goods as preventive care: one state is an N of 1 and we love and need our state and local public health departments. But viruses and foodborne illnesses don’t really care about ZIP or postal codes in an open and free society.
And a lot of us really do need that data to get our work done…..let alone keep research going for curing diseases, get preventive services and medicines to people who don’t have to succumb to preventable death and disability. Scale matters in public health (which is a real thing).


 Thank you
Thank you  Jane joined host Dr. Geeta "Dr. G" Nayyar and colleagues to brainstorm the value of vaccines for public and individual health in this challenging environment for health literacy, health politics, and health citizen grievance.
Jane joined host Dr. Geeta "Dr. G" Nayyar and colleagues to brainstorm the value of vaccines for public and individual health in this challenging environment for health literacy, health politics, and health citizen grievance.