
Even though women comprise one-half of the world’s population, their health outcomes and inputs do not match up to men’s: there’s a women’s health gap on Planet Earth.
Meeting in Davos this week for #WEF2025, the World Economic Forum published a report on that gender-health chasm titled, Blueprint to Close the Women’s Health Gap: How to Improve Lives and Economies for All.

In collaboration with the McKinsey Health Institute, the report focuses on nine key conditions that, if addressed, could reduce the global disease burden by 27 million disability adjusted life years and add 2.5 healthy days per woman per year. This would add $400 billion of “economic uplift,” improving the lives of women worldwide.
And that economic uplift is the fiscal meaning of “Health is Wealth.”
This report follows up last year’s WEF study on women’s health disparities, Closing the Women’s Health Gap: A $1 Trillion Opportunity to Improve Lives and Economies. The study team leader’s introductory note for this year’s update calls out that last year’s version, “tapped into what many readers instinctively felt: when it comes to health, women are second-class citizens.”

In the 2025 update, we get more granular data from which the WEF and McKinsey collaborators can develop the blueprint for action.
The research analyzed data from 15 countries across four income archetypes based on World Bank data; these countries reflect different health care systems and socioeconomic profiles. (You can read more on the methodology in detail in the appendix of the report).
Nine health conditions were included in the research which are key contributors to the gender health gap which impact women’s burden of disease in terms of disability-adjusted life years (DALYs) and other outcome metrics:
- Affecting lifespan: breast cancer, cervical cancer, ischaemic heart disease, maternal hypertension, and post-partum haemorrhage; and,
- Affecting health span: endometriosis, menopause, migraine, and pre-menstrual syndrome (PMS).

Underneath the gaps by disease are five factors that drive the health disparities: they are characterized by five action verbs which, if addressed together, would help to ameliorate the health disparities between women of the world compared with men. The “action verbs” are,
- To count women in terms of data collection
- To study women in terms of funding research focused on female-specific health issues
- To care for women deploying contemporary clinical guidelines and best practices
- To include all women, embracing historically marginalized communities; and,
- To invest in women, for allocating more funds to designing and implementing accessible care and delivery models for services.
The report details each of these five areas and tactics for addressing counting, studying, caring for, including, and investing in women — to close the gender health gaps seen around the world.

Take just one of dozens of areas of opportunity profiled in the latter half of the report to help close the chasm of women’s health disparities: clinical trials.
This bar chart from the study illustrates “where” women’s health research is concentrates, and then where the disability burden is pronounced for that clinical area. Where more trials are funded in higher income countries, but burden of disease is greater in lower-income nations. On average across the nine conditions, the burden overall is 54% in lower-income countries, but the percent of clinical trials in these countries is only 23%.
For example, check out the huge gap in post-partum hemorrhage: 90% of the burden (measured in DALYs) occurs in lower income nations, but most of the clinical trials for the condition happen in higher-income countries. This pattern is true across the nine conditions.
Health Populi’s Hot Points: “Global health and social systems were not designed around the health of women,” the conclusion of the WEF report begins. Women face barriers to care, see providers who lack knowledge of women-specific health issues, and are at greater risk of premature death and avoidable disability.
Solving this challenge will take more than a village: it will require a cross-sectoral approach between sectors — private, public, and social — to bring to bear each of their skills, funding pools, and cultural expertise in assuring programs are designed for women (and hopefully by women in the process). In the private sector, we should be inclusive — bringing into solutions business, investors, philanthropies, and universities, all of whom have gifts of all flavors to bring to the solution sets.
As an end-note, in conversations I’ve had with colleagues and friends who attended #JPM2025 in San Francisco, there were continued gaps in funding women’s health start-ups and companies led by women in general. This is a long-time challenge which has anecdotes of bright spots but still a through-line that’s stubbornly sticky. In one of her last public speeches as First Lady of the United States, Dr. Jill Biden spoke at the JPM meeting on a special track addressing women’s health. 
“Women are waiting for better answers to improve their health, and the potential in this space is too great to ignore,” Dr. Biden said. “I’m so proud that the White House Initiative on Women’s Health Research has laid down a new marker of progress, but that new standard isn’t the finish line for me, it’s my starting point,” she noted.
This witty and insightful post written by veteran health care investor and strategist Lisa Suennen, the Venture Valkyrie (and my BFF), will give you a rich sense of the #JPM2025 meeting and how it has evolved since its early days which Lisa has witnessed herself for 3 decades — with a rich assessment of how women’s health and investing in it has evolved over the years.
We can connect these dots to the larger issue of women’s health disparities, again returning to the cross-sector solutions bringing together diverse funders and imagineers who can/must converge for the benefit of the world’s women.
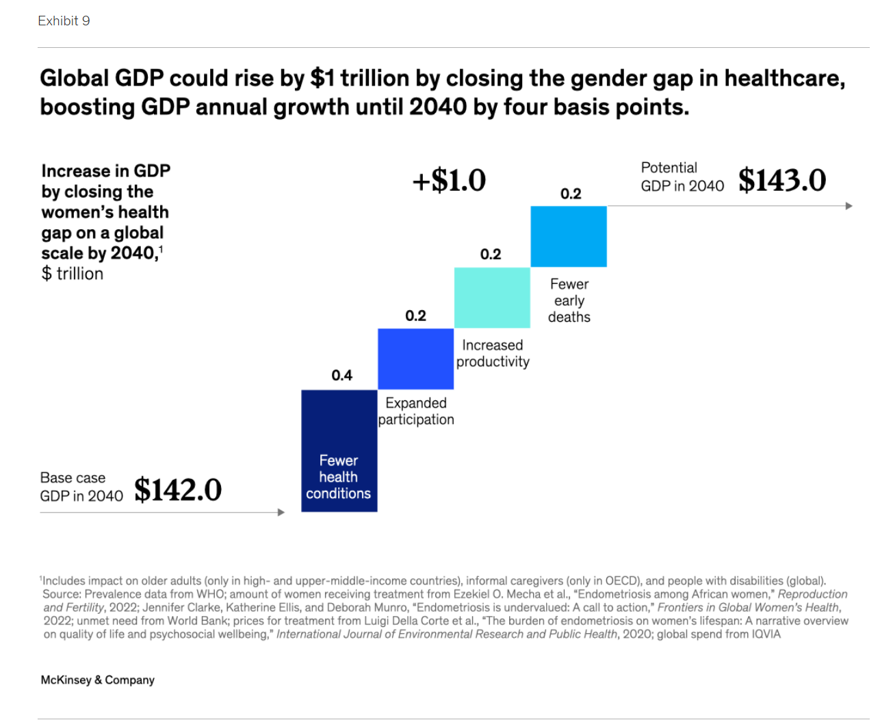
As the last chart from last year’s report illustrates, the economic benefits of closing the women’s health gap are compelling at scale.


 I'm gratified to be named on
I'm gratified to be named on  I’m celebrating America’s 250th birthday both patriotically and professionally, honored that the NLM included my 2010 paper, “How Smartphones Are Changing Healthcare for Consumers and Patients” as one of 250 items curated for the digital archive of 250 Years of American Medicine.
I’m celebrating America’s 250th birthday both patriotically and professionally, honored that the NLM included my 2010 paper, “How Smartphones Are Changing Healthcare for Consumers and Patients” as one of 250 items curated for the digital archive of 250 Years of American Medicine.